You deserve a second chance — done right this time.
Specialized revision rhinoplasty by a double board-certified plastic surgeon (FACS & FEBOPRAS). Structural reconstruction of failed primary nose surgery — from over-resection to nasal collapse — with cartilage grafts when needed.
According to the American Academy of Facial Plastic and Reconstructive Surgery, revision surgery numbers have nearly doubled since 2017. Roughly 5-15% of primary rhinoplasty patients eventually seek revision. Understanding why helps avoid the same mistakes the second time.
Surgeon-related causes
·Inexperience — Rhinoplasty is the most technically demanding facial procedure. Surgeons performing only a handful per year cannot consistently deliver natural results.
·Over-resection — Removing too much cartilage or bone creates collapsed tip, scooped bridge, or pinched appearance that ages poorly.
·Insufficient internal support — Reduction without reinforcement causes airway collapse and breathing difficulty 5-10 years later.
·Generic planning — One technique applied to all patients regardless of skin thickness, ethnic anatomy, or facial harmony.
·Non-core providers — ER doctors, general practitioners, or unqualified staff performing rhinoplasty have produced a sharp rise in botched outcomes.
Patient-related & healing factors
·Unrealistic expectations — Photos of celebrities or filtered images set goals incompatible with the patient's actual anatomy.
·Skin recovery variability — Thick sebaceous skin or a tendency to form excessive scar tissue can mask refinements that were technically performed correctly.
·Poor post-operative compliance — Trauma, smoking, or returning to contact activity too early can disrupt healing.
·Late tissue changes — Cartilage memory can return over years; reduction-only techniques are particularly vulnerable to long-term shape change.
·Communication failure — When patient goals and surgical plan don't truly align, the result can be technically correct but personally disappointing.
Most common revision triggers
Aesthetic
Pinched tip · scooped bridge · polly-beak · saddle nose · persistent hump · asymmetry · over-rotated tip · droopy tip
Functional
Internal valve collapse · breathing obstruction · whistling on inhalation · chronic crusting · sinus issues · loss of nasal support
Combined
Most revision cases involve both aesthetic and functional issues — the structures that hold shape also support airflow.
Reality check — Not every dissatisfaction is a botched surgery. Studies show 5-10% of patients want minor refinements (slightly more refined tip, fine-tuning a deviation) — these are often considered enhancement revisions, not corrections of failure. Distinguishing between the two is the first step in honest planning.
My Revision Approach
Structural reconstruction, not more reduction
Most failed primaries fail because too much was removed. Revision rhinoplasty is fundamentally different — the goal is to rebuild what was lost, support what remains, and restore both shape and function. Reduction-on-reduction almost always makes things worse.
·Cartilage graft strategy — Septal cartilage if available, ear (auricular) for moderate cases, rib (costal) for major reconstruction. Choice driven by what your case requires, not surgeon preference.
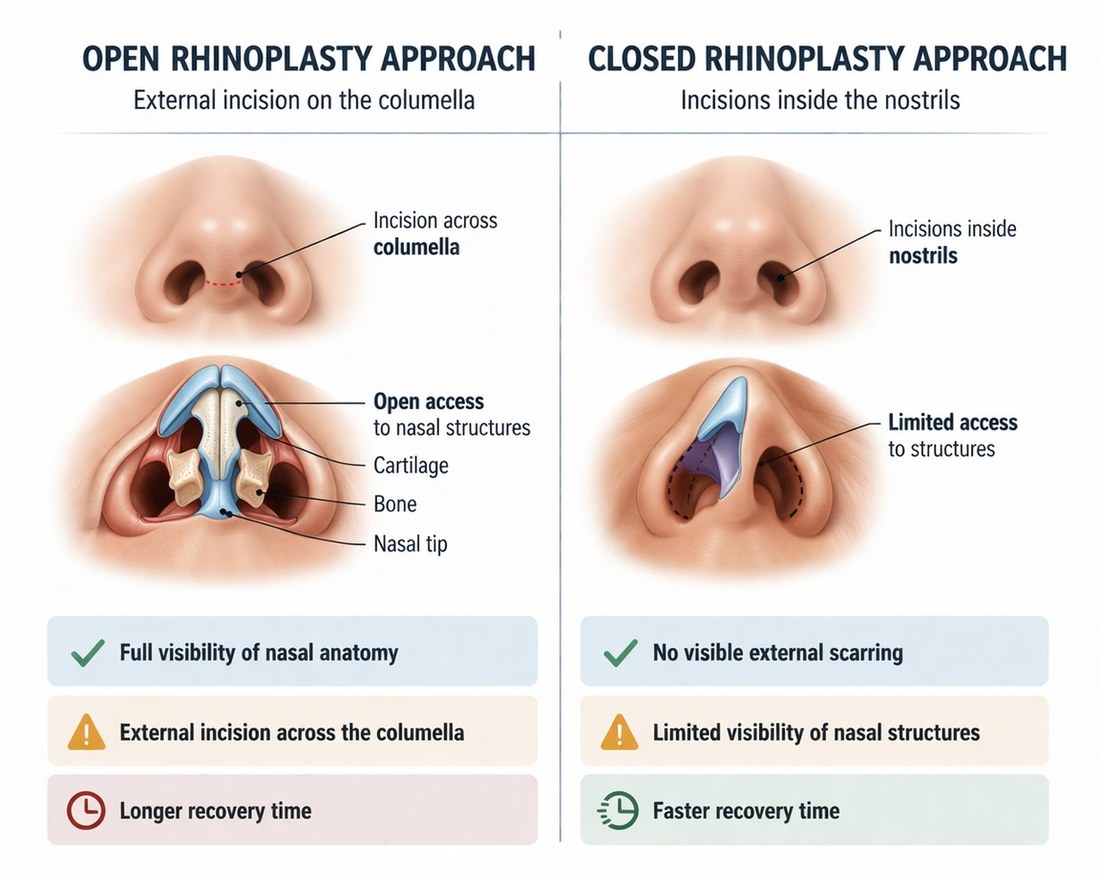
·Closed approach when possible — Many revisions can still be performed through internal incisions only (no external scar). Open approach is reserved for cases that genuinely need it.
·Spreader grafts & struts — Internal support structures that prevent late collapse and restore breathing function.
·Diced cartilage in fascia (DCF) — For dorsal contour smoothing, especially on thin-skinned patients where graft visibility is a risk.
·Realistic stage planning — Some severe cases benefit from staged surgery (e.g. tissue expansion before grafting) rather than attempting everything at once.
·Scar tissue management — Dense adhesions from previous surgery require careful dissection and sometimes scar release with steroid injection adjunct.
Reduction vs Reconstruction
Old-school rhinoplasty focused on removing tissue. Modern revision focuses on supporting and rebuilding it. The shift in philosophy is the single most important advance in revision outcomes over the past two decades.
REDUCTION
Take away · weakens support · ages poorly · hard to revise
STRUCTURE
Add support · maintains shape · ages well · easier to revise if needed
Common Revision Cases
What I see in revision consultations
Each deformity has its own surgical signature — and its own correction strategy. Here are the patterns I encounter most often in revision evaluations.
Aesthetic · Tip
Pinched tip
Over-narrowed nasal tip from excessive cartilage removal. Looks unnatural in profile, often impacts breathing. Correction: lateral crural strut grafts to rebuild width and support.
Aesthetic · Bridge
Scooped (ski-slope) bridge
Over-resected dorsum — the bridge looks visibly concave from profile view. Especially feminizing, often unwanted. Correction: dorsal augmentation with diced cartilage or onlay graft.
Aesthetic · Profile
Polly-beak deformity
Fullness in the supratip area giving a parrot-beak profile. Caused by inadequate dorsum lowering, scar tissue, or weak tip support. Correction depends on cause — soft tissue, cartilage, or both.
Structural · Severe
Saddle nose deformity
Collapsed middle vault from septal cartilage loss. Often follows aggressive septoplasty or hematoma. Correction: structural rebuild typically requires rib cartilage grafts.
Functional
Internal valve collapse
Breathing difficulty, especially on deep inhalation. The middle vault narrows excessively. Correction: spreader grafts to widen and support the internal valve.
Aesthetic · Asymmetry
Crooked / deviated nose
Either persistent from before primary surgery or new asymmetry. Often combined with septal deviation. Correction: extracorporeal septoplasty or septal stabilization with battens.
Every revision case has its own story — over-resection rebuilt with grafts, breathing restored after valve collapse, asymmetry corrected after the first surgery's mistakes. Real photos of real revision patients, with surgical context for each case.
All photos are real revision patients who gave written consent for educational publication. Identifiers are coded (#186, #242…) for privacy and every image is watermarked. Photos range from 6 days to 3 months post-op — these are mid-stage healing, not final outcomes. Final refinement continues through 18–24 months, and individual results vary by anatomy and primary-surgery history.
Revision Timing
When can I have revision rhinoplasty?
The single biggest mistake in revision planning is acting too soon. The nose continues to settle, scar tissue softens, and the "final result" of the primary surgery becomes apparent only after 12 months.
0-6 months
Wait — don't act
Heavy swelling, especially in tip and supratip. Many "deformities" at this stage are temporary swelling that will resolve on its own.
6-12 months
Evaluate, plan
Send photos for revision consultation. Discuss strategy. Order CT or 3D imaging if needed. But still don't operate yet.
12+ months
Surgical window
Tissues fully healed, scar tissue softened, accurate planning possible. Most revisions performed at 12-18 months from primary surgery.
Emergency
Exception only
Earlier intervention only for: infection, airway emergency, displaced graft. Aesthetic concerns alone never justify rushing.
A note on impatience — I understand the urgency. Living with a result you dislike is hard, especially seeing it daily. But revision performed too early routinely produces worse results than revision performed at the right time. The waiting is part of getting it right.
Revision Rhinoplasty Cost
Honest pricing for complex work
Revision rhinoplasty costs more than primary because it takes longer, demands greater expertise, and often requires cartilage harvest from a second site. Here's how my pricing works — and how it compares globally.
My revision packages — Istanbul (2026)
Standard revision
from €4,500
Tip refinement, dorsal smoothing, ear cartilage if needed, asymmetry correction. Closed approach when possible.
Complex revision
€5,500-7,000
Multiple grafts, internal valve repair, septoplasty component, scar tissue management. May require open approach.
Istanbul revision savings: 60-75% versus US/UK — at equivalent or higher surgical expertise. The price difference reflects Turkey's lower operational costs, not lower standards.
From the first photo evaluation to the final 12-month follow-up, every step is coordinated. International patients fly in, recover in luxury, and return home with structured remote follow-up.
Step 1
📸
Photo evaluation (free)
Send photos of your nose from front, profile (both sides), oblique, and base view. Include your previous operative reports if available. I personally review every consultation request and respond within 24 hours with an honest case assessment.
Step 2
💬
Video consultation
A 30-45 minute WhatsApp or Zoom call. We review your photos together, discuss what went wrong with the primary, set realistic goals, and outline the surgical strategy. No pressure to commit — many patients consult and decide later.
Step 3
✈️
Travel to Istanbul
Direct VIP transfer from airport to your luxury hotel. Day 1 is rest. Day 2: in-person consultation, photo documentation, anesthesia clearance, surgical planning finalization. Day 3: surgery.
Step 4
🏥
Surgery (3-5 hours)
Performed in JCI-accredited private hospital under general anesthesia by certified anesthesiologist. Operative time depends on complexity — simple revision 2-3 hours, complex with rib graft 4-5 hours. One night hospital observation.
Step 5
🛏️
Hotel recovery
Days 4-9 in luxury hotel. Daily check-ins by clinic team. Splint removal at day 7. By day 10, most patients are presentable enough for return travel. Detailed written aftercare instructions in your language.
Step 6
📲
12-month remote follow-up
Video check-ins at 1 month, 3 months, 6 months, and 12 months. Photo monitoring. Written reports for your local doctor. Final result evaluation at 12-18 months — revision results take longer to mature than primary.
Where you stay — luxury hotel
5-star hotel in central Istanbul. Concierge service, daily breakfast, premium amenities. Room blocks reserved for international patients.
5-star rating
Central Istanbul
Concierge service
Premium bedding
Quiet environment
Reliable Wi-Fi
Daily breakfast
English staff
About the Surgeon
Dr. Ayhan Işık Erdal — FACS, FEBOPRAS
Associate Professor of Plastic Surgery at Gazi University. Double board-certified — Fellow of the American College of Surgeons (FACS) and Fellow of the European Board of Plastic, Reconstructive and Aesthetic Surgery (FEBOPRAS). Over 2,000 rhinoplasty procedures performed, including a substantial revision practice attracting referrals from across Europe and the Gulf.
My academic work spans 30+ peer-reviewed publications in plastic surgery journals. Active member of ISAPS, TSPRAS, and the European Rhinology Society. I regularly lecture at international congresses on revision rhinoplasty technique, particularly on cartilage graft strategies and structural reconstruction.
Why I focus heavily on revision work: when a primary fails, the patient bears the cost — emotionally, financially, and in trust. Doing revision well requires both technical mastery and the patience to plan staged solutions. Most of my revision patients have already had one or two surgeries elsewhere; I take that history seriously.
Most surgeons recommend waiting 12 months. Tissues need to fully heal, swelling needs to resolve, and the final result of the primary surgery needs to settle before accurate planning can be made. Earlier revision is reserved for emergencies — infection, airway obstruction, displaced graft.
My revision packages range from €4,500 (standard refinement) to €8,500 (major reconstruction with rib graft). This is significantly more affordable than the US ($15,000-30,000) or UK (£8,000-15,000) for comparable expertise. All-inclusive — surgery, hotel, transfers, follow-ups.
Revision rhinoplasty is technically more complex due to scar tissue from the first surgery, distorted anatomy, depleted septal cartilage requiring grafts from ear or rib, and longer operative times (3.5-5 hours vs 2 hours for primary). It demands a surgeon with specific revision experience.
Not always. Many revisions can be done using ear cartilage or remaining septum. Rib is reserved for cases requiring substantial structural rebuild — saddle deformity, severe collapse, or third revisions. The decision is based on what your case actually needs.
Many revisions can be performed through a closed (endonasal) approach. Complex structural revisions sometimes benefit from open access. I select technique based on what your case requires — not a one-size-fits-all preference. If your previous surgery was open, the existing scar can typically be used.
When performed by an experienced revision specialist, success rates range from 85-95%. Revision is inherently more complex than primary, and a small percentage of patients (5-10%) may need further refinements. Realistic expectations and stage-by-stage planning are essential.
Initial recovery is similar to primary — splint removed at 7 days, social-presentable at 2-3 weeks. But final result maturation takes 12-18 months versus 12 for primary. Scar tissue and graft integration extend the timeline. Patience is essential.
Operative reports are useful but not essential. Through clinical examination, photo analysis, and CT imaging when needed, the previous surgical pattern can usually be reconstructed. If your previous surgeon is uncooperative, this is unfortunately common — and not a barrier to your revision.
Send 4-5 photos of your nose (front, profile both sides, oblique, base view) along with your previous surgery details. I'll personally review and respond within 24 hours with an honest assessment — including whether revision is indicated, when, and approximate cost range.